This is an expanded version of my chat about AHS2014 over at the Efficient Exercise blog. Go read that now if you haven’t yet…I’ll wait.
…Good? Good.
If you haven’t seen the video, you can take a look at that too:
So in addition to everything I wrote over there and said in my talk, there are a few small additions I’d like to make about the event. First of all, the thing that is readily apparent from year one (2011) to year four is that the organizers have started to separate the wheat from the chaff, so to speak. For example, Year one featured talks about the topic of violence in the course of human evolutionary history, which is actually not an unrelated or topic lacking in discussion (for example, see Ned’s exploration of the War of Canudos and the unexpected longevity of the survivors). However, from the perspective things a person can control or influence, famine and war are so far away from either. So AHS has moved from the total umbrella of things that have influenced evolutionary outcomes to the things that we can control or influence that lead to larger health & healthcare outcomes. Further, you had to present your evidence for your conclusions. It wasn’t enough to present a just so description, but rather people gave guided tours of the science and how it doesn’t fit perfectly with what is currently recommended, either in the ancestral health community or in the mainstream community. As I said before: You had to show your work.
So what would I have added? Well, the one point I forgot to expand upon was something I was actually criticized for: it kinda looks like a HIT protocol is the “best” for achieving these outcomes. The point I wanted to make, and simply forgot, is that like the rest of the evidence base, there is no “base protocol” for testing to see if certain putative markers or clinically significant outcomes are even seen in humans (based on animal studies).
This exists for cardiorespiratory training. Are you familiar with the Bruce protocol? On a treadmill, you increase the speed and grade until a person taps out or a true VO2 max is reached:
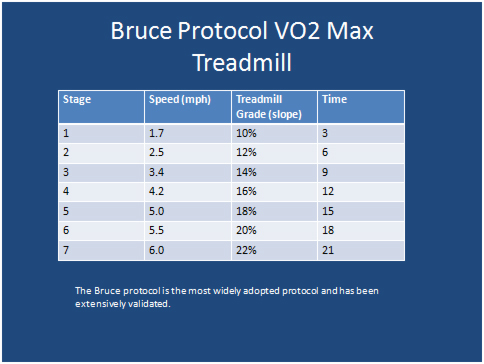 So this is normally used as a stress test (“Graded Exercise Test”) to determine some amount of metabolic fitness. As we learned in school, it’s also a dismissal test that is done with EKG so if the person kicks in the parking lot, you have data to show that they were great on the treadmill!
So this is normally used as a stress test (“Graded Exercise Test”) to determine some amount of metabolic fitness. As we learned in school, it’s also a dismissal test that is done with EKG so if the person kicks in the parking lot, you have data to show that they were great on the treadmill!
Anyway, when a novel marker of something is discovered in animal models, a standardized test like this is helpful to see if said marker is seen in humans. For example, here’s a clinical trial in which the Bruce will be used to see if BDNF is increased in those with spinal cord injury. What I’d like to see is someone put together, based on the literature, the resistance training equivalent to the Bruce, one that can be used to determine physiological responses to a particular training modality. This does not imply that it is the only protocol that elicits the response; it’s only there to test the feasibility of response.
In other words, the exercise physiologists had to go through the Bruce before getting to Tabata as far as determining changes in lactate threshold (for example). The same thing needs to occur for resistance training: a base protocol that determines IF a change can occur before the variables are tweaked as to how to MAXIMIZE the change that occurs.
So, you know, if that looks like HIT currently, so be it. I can’t turn an ought into an is, no matter how confident you are that it’s sub-optimal. That’s why we do research, folks, but you gotta start at square one.

You say that it kind of looks like an HIT protocol is best for achieving these outcomes. Yet the prescription that you showed in the talk looked like a more conventional resistance training regime (3 sets of 10, 6-12 exercises, 2-3 times a week). And this prescription came form the meat (or fat part?) of the studies. So I’m confused about the basis for saying HIT might be better than the prescription shown in the talk for these sorts of brain improvements.
Have any studies compared high intensity of effort versus high intensity of load for these kind of cognitive improvements? I imagine it might be hard to differentiate since if you exercise at a high intensity of load, and continuously try to progress the weight, then you will always end up with sets that end at a high intensity of effort.
Hey Skyler,
How’s it going? Wondering what your training frequency is like these days – still once every 5? Are you still doing mostly SS HIT with some old school weights thrown in? Still doing chaos training? How about diet – still paleo with carb cycling on workout days? or have you added safe starches? Also, how’s the HRV going?
Good to hear from you.
Best,
Scott